MACE Practice Exam - Medication Aide Certification Examination
Reliable Study Materials & Testing Engine for MACE Exam Success!
Exam Code: MACE
Exam Name: Medication Aide Certification Examination
Certification Provider: Test Prep
Certification Exam Name: Test Prep Certifications


Free Updates PDF & Test Engine
Verified By IT Certified Experts
Guaranteed To Have Actual Exam Questions
Up-To-Date Exam Study Material
99.5% High Success Pass Rate
100% Accurate Answers
100% Money Back Guarantee
Instant Downloads
Free Fast Exam Updates
Exam Questions And Answers PDF
Best Value Available in Market
Try Demo Before You Buy
Secure Shopping Experience
MACE: Medication Aide Certification Examination Study Material and Test Engine
Last Update Check: Mar 19, 2026
Latest 311 Questions & Answers
45-75% OFF
Hurry up! offer ends in 00 Days 00h 00m 00s
*Download the Test Player for FREE
Dumpsarena Test Prep Medication Aide Certification Examination (MACE) Free Practice Exam Simulator Test Engine Exam preparation with its cutting-edge combination of authentic test simulation, dynamic adaptability, and intuitive design. Recognized as the industry-leading practice platform, it empowers candidates to master their certification journey through these standout features.
What is in the Premium File?
Satisfaction Policy – Dumpsarena.co
At DumpsArena.co, your success is our top priority. Our dedicated technical team works tirelessly day and night to deliver high-quality, up-to-date Practice Exam and study resources. We carefully craft our content to ensure it’s accurate, relevant, and aligned with the latest exam guidelines. Your satisfaction matters to us, and we are always working to provide you with the best possible learning experience. If you’re ever unsatisfied with our material, don’t hesitate to reach out—we’re here to support you. With DumpsArena.co, you can study with confidence, backed by a team you can trust.
Test Prep MACE Exam FAQs
Introduction of Test Prep MACE Exam!
The MACE (Master of Arts in Counseling Examination) is a comprehensive exam used to assess the knowledge, skills, and abilities of those seeking licensure as a professional counselor. It covers topics such as professional identity, counseling theory and techniques, ethical and legal issues, and human growth and development.
What is the Duration of Test Prep MACE Exam?
The duration of the Test Prep MACE Exam is 3 hours.
What are the Number of Questions Asked in Test Prep MACE Exam?
The exact number of questions in the Test Prep MACE Exam varies depending on the specific exam you are taking. According to the Test Prep MACE website, each exam generally consists of 50-75 multiple-choice questions.
What is the Passing Score for Test Prep MACE Exam?
The passing score required for Test Prep MACE depends on the institution or program you are seeking admission to. Each institution or program has its own criteria for determining the minimum passing score. Generally, there is no official passing score for Test Prep MACE, however, a score of 70% or higher is usually considered a passing score.
What is the Competency Level required for Test Prep MACE Exam?
The Competency Level required for the Test Prep MACE exam is a minimum of Intermediate.
What is the Question Format of Test Prep MACE Exam?
The MACE exam consists of multiple-choice questions.
How Can You Take Test Prep MACE Exam?
The Test Prep MACE exam can be taken either online or in a testing center. To take the exam online, you will need to register and purchase the exam on the Test Prep MACE website. Once you have registered and paid, you will receive an email with instructions on how to access the exam. To take the exam in a testing center, you will need to contact the Test Prep MACE office to find out the closest testing center and to register for the exam.
What Language Test Prep MACE Exam is Offered?
The MACE exam is offered in English.
What is the Cost of Test Prep MACE Exam?
The cost of the MACE exam varies depending on the testing center. Generally, the cost ranges from $50 to $90.
What is the Target Audience of Test Prep MACE Exam?
The target audience of Test Prep MACE Exam is students who are preparing for the MACE exam. This exam is designed for students who are looking to become certified as a medical assistant. It is also suitable for students who are looking to gain a better understanding of the medical assistant profession and the skills and knowledge needed to be successful in the field.
What is the Average Salary of Test Prep MACE Certified in the Market?
The average salary in the market after Test Prep MACE exam certification varies depending on the individual's experience, skills, and location. Generally speaking, individuals who have completed the Test Prep MACE exam certification can expect to earn an average salary of around $50,000 per year.
Who are the Testing Providers of Test Prep MACE Exam?
The Test Prep MACE exam is administered by the National Board for Certified Counselors (NBCC). The NBCC offers testing through its network of authorized test sites. To find a testing site near you, visit the NBCC website and use the “Find a Test Site” tool.
What is the Recommended Experience for Test Prep MACE Exam?
The recommended experience for Test Prep MACE Exam is to have a good understanding of the topics covered in the exam, such as math, English, reading, and writing. It is also recommended to have a good understanding of the exam format and the types of questions that are asked. Additionally, it is important to have a good study plan and practice test taking strategies. Finally, it is beneficial to review the material covered in the exam and to practice taking the exam under timed conditions.
What are the Prerequisites of Test Prep MACE Exam?
The Prerequisite for Test Prep MACE Exam is that you must have a valid high school diploma or GED. You must also be at least 18 years old.
What is the Expected Retirement Date of Test Prep MACE Exam?
The official website for the Test Prep MACE exam is https://www.testprepreview.com/mace-test-preparation.html. There is no official information regarding the expected retirement date of the exam.
What is the Difficulty Level of Test Prep MACE Exam?
The difficulty level of the Test Prep MACE exam can vary depending on the student's knowledge and experience. Generally, the exam is considered to be of moderate difficulty.
What is the Roadmap / Track of Test Prep MACE Exam?
The certification roadmap for the Test Prep MACE Exam is as follows:
1. Complete the Test Prep MACE Exam Prep Course.
2. Take the Test Prep MACE Exam.
3. Receive your Test Prep MACE Exam Certification.
4. Maintain your Test Prep MACE Exam Certification by completing continuing education requirements.
5. Renew your Test Prep MACE Exam Certification every two years.
What are the Topics Test Prep MACE Exam Covers?
Test Prep MACE exam covers a variety of topics related to college admissions and test preparation. These topics include:
1. College Admissions: This section covers topics related to the college admissions process, including college selection criteria, application strategies, financial aid, and more.
2. Test Prep: This section covers topics related to test preparation, including test taking strategies, test structure, and other test-related topics.
3. Academic Skills: This section covers topics related to academic skills, including time management, study skills, note-taking, and more.
4. Writing: This section covers topics related to writing, including essay structure, grammar, and other writing-related topics.
5. Mathematics: This section covers topics related to mathematics, including algebra, geometry, calculus, and other math-related topics.
6. Science: This section covers topics related to science, including biology, chemistry, and other science-related topics.
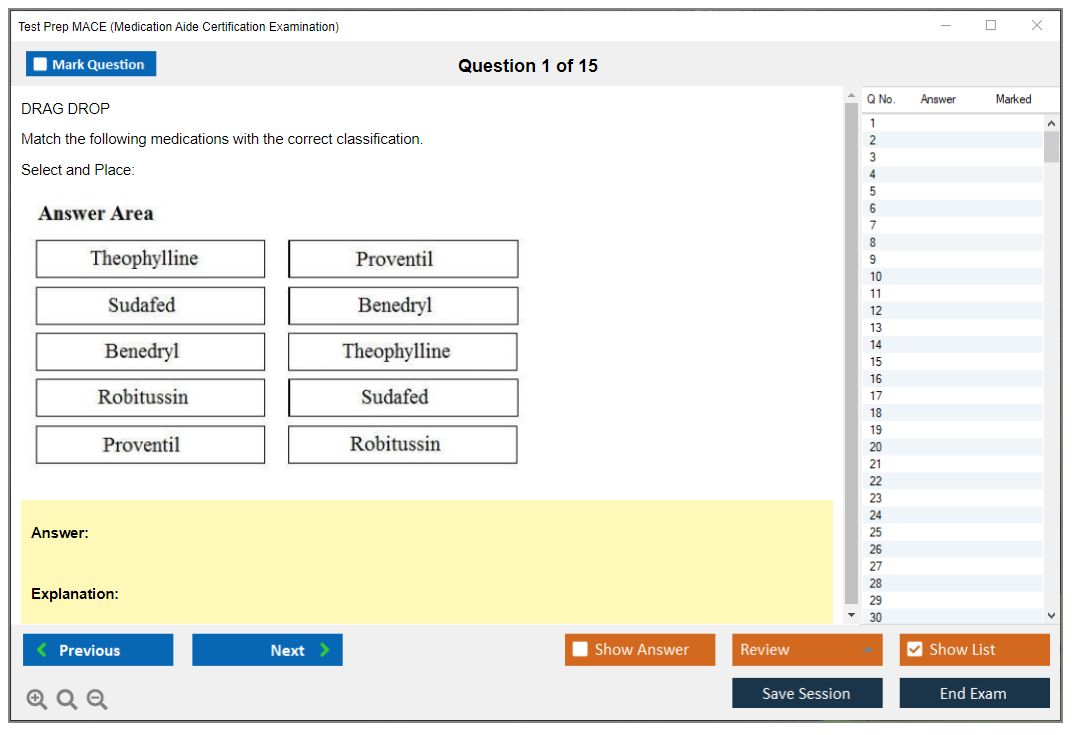
What are the Sample Questions of Test Prep MACE Exam?
1. What is the definition of MACE?
2. What types of tests are included in the MACE exam?
3. What are the benefits of taking the MACE exam?
4. What is the format of the MACE exam?
5. What topics are covered on the MACE exam?
6. How is the MACE exam scored?
7. What is the passing score for the MACE exam?
8. What is the time limit for the MACE exam?
9. What resources are available to help prepare for the MACE exam?
10. What are the consequences of failing the MACE exam?
What Is the MACE (Medication Aide Certification Examination)? What exactly is the MACE and why it matters in healthcare The Medication Aide Certification Examination is a standardized competency test proving you can safely administer medications under a licensed nurse's supervision. Not a nursing license. Not even close, honestly. But it opens doors for unlicensed assistive personnel who want more than just basic patient care without committing to a full LPN or RN program. Look, the healthcare field desperately needs people handling medication administration in long-term care settings. Nurses are stretched thin, and certified medication aides fill a gap by taking on routine medication passes while nurses focus on assessments and clinical decisions that actually require their license. The Test Prep MACE (Medication Aide Certification Examination) validates that you understand the five (or six, depending on who's teaching) rights of medication administration, can document properly, and... Read More
What Is the MACE (Medication Aide Certification Examination)?
What exactly is the MACE and why it matters in healthcare
The Medication Aide Certification Examination is a standardized competency test proving you can safely administer medications under a licensed nurse's supervision. Not a nursing license. Not even close, honestly. But it opens doors for unlicensed assistive personnel who want more than just basic patient care without committing to a full LPN or RN program.
Look, the healthcare field desperately needs people handling medication administration in long-term care settings. Nurses are stretched thin, and certified medication aides fill a gap by taking on routine medication passes while nurses focus on assessments and clinical decisions that actually require their license. The Test Prep MACE (Medication Aide Certification Examination) validates that you understand the five (or six, depending on who's teaching) rights of medication administration, can document properly, and know when something's going wrong.
State boards of nursing or their designated testing agencies typically administer the exam. Some states use the National Council of State Boards of Nursing (NCSBN) version, others developed their own, and a few contract with testing companies. The result? You've got state-specific variations that can drive you absolutely crazy if you're trying to transfer your certification across state lines, but the core competencies remain pretty consistent: safe med admin, proper documentation, recognizing problems, and staying within your scope.
Who needs this certification and why they're pursuing it
Certified nursing assistants looking to expand what they can do at work make up the biggest chunk of test-takers. You've been doing vitals, bathing, feeding, and transferring patients for a while, and now you want the authority to pass meds without waiting for an LPN to show up. Makes total sense. The pay bump isn't huge in most facilities. Maybe an extra dollar or two per hour. But it makes you more valuable and harder to replace.
Unlicensed assistive personnel in long-term care, assisted living, group homes, and residential care facilities increasingly need this credential just to keep their current jobs. Many states have moved from optional to mandatory certification over the past decade as regulators got more serious about medication safety. I mean, if you're handing someone their heart medication, diabetes pills, and blood thinners, probably good to prove you know what you're doing.
Home health aides pursuing medication administration privileges represent another growing group. Clients at home need their meds just like residents in facilities, but oversight's trickier. The assisted living medication aide certification pathway often overlaps with MACE requirements, though some states differentiate between institutional and home-based settings.
Career changers entering healthcare through the medication aide route like the relatively short training period compared to nursing school. You can complete the required coursework and clinical hours in a few weeks to maybe a couple months, sit for the exam, and start working in a specialized role. It's not the same career trajectory as becoming a nurse, obviously, but it's a legitimate entry point that doesn't require years of prerequisites and clinicals. My cousin took this route after years managing a retail store, and she's never looked back, though she complains about the smell sometimes.
What the certification actually lets you do on the job
Administering oral medications is your bread and butter. Tablets, capsules, liquids, sublingual medications. You'll be crushing pills for residents with swallowing difficulties (when appropriate), mixing liquid meds, and documenting everything on the medication administration record. The MAR documentation and medication errors section of your training will hammer home why accurate charting matters, because if you didn't document it, you didn't do it, and that's how people get double-dosed.
Topical medications fall within most medication aides' scope: creams for skin conditions, antibiotic ointments, transdermal patches for pain or nicotine replacement, medicated shampoos. You'll also instill eye drops for glaucoma or infections, ear drops for wax or infections, and nasal sprays or drops. Some states allow rectal suppositories and vaginal medications, others don't. State rules here get really granular.
Monitoring for therapeutic effects and adverse reactions is part of the job that textbooks underemphasize but real-world practice demands constantly. You're watching for whether the blood pressure medication is actually lowering blood pressure, whether the pain medication's working, whether someone's getting drowsy from their new antianxiety med. When something seems off (new confusion, rash, difficulty breathing, weird behavior), you report to the supervising nurse right away.
Documentation responsibilities extend beyond the MAR, honestly. Incident reports for medication errors, notes about refused medications, observations about side effects, controlled substance counts and logs if your facility handles them through medication aides. The safe medication administration training you receive should hammer home that documentation protects both patients and you legally.
Scope limitations vary wildly by state and you absolutely must know yours. Most states prohibit medication aides from administering injectable medications except in very specific circumstances. Some allow insulin after additional training, most don't. IV medications are universally off-limits. PRN (as-needed) medications might require extra certification or might be completely restricted to nurses. Settings matter too. Your scope in a nursing home might differ from your scope in assisted living or a group home.
How MACE differs from other healthcare credentials
The Medication Aide Certification Exam prep targets a much narrower skill set than a CNA exam. CNA certification covers all basic nursing assistant skills: transfers, bathing, feeding, key signs, communication, patient rights. MACE assumes you already have those foundational skills and tests specifically on medication-related competencies. Many states actually require current CNA certification as a prerequisite for taking MACE.
Compared to LPN or RN programs, medication aide training is radically shorter and less full, which is kind of the point. LPNs can assess patients, develop care plans, start IVs in most states, and work relatively independently. RNs have even broader scope. Medication aides work under direct delegation from licensed nurses and can't make independent clinical judgments about medication appropriateness. You're implementing orders, not evaluating them.
Pharmacy technician certification covers completely different territory. Filling prescriptions, insurance billing, inventory management, compounding. Pharmacy techs work in retail and institutional pharmacies under pharmacist supervision. Medication aides work in direct patient care settings under nurse supervision. The pharmacology knowledge overlaps somewhat, but the day-to-day job functions are totally different.
The legal framework governing medication aides centers on delegation. A licensed nurse must assess each resident, determine that medication administration can be safely delegated for that specific resident and medication, delegate the task to a certified medication aide, and supervise the process. This isn't a blanket "you can give all meds to everyone" situation. It's supposed to be individualized and ongoing, though in practice many facilities treat it more broadly than regulations technically allow.
Career possibilities after certification
Immediate employment opportunities in long-term care facilities represent the most common path. Nursing homes, skilled nursing facilities, and rehabilitation centers employ the majority of certified medication aides. You'll work med passes (typically morning, noon, evening, and bedtime rounds) along with documentation and monitoring duties.
Assisted living facilities and residential care homes increasingly require medication aide certification for staff who help residents with medications. The environment tends to be less clinical than nursing homes, residents are generally more independent, but medication needs are still significant. Some people prefer this setting because it feels less institutional, more like actual homes.
Group homes for individuals with developmental disabilities or mental health conditions employ medication aides to ensure residents take prescribed medications correctly. These settings often involve smaller groups of residents and more individualized attention, though behavioral challenges can make the work demanding in different ways.
Career advancement from medication aide typically means pursuing LPN or RN licensure. Some people use medication aide certification as a stepping stone to test whether they want to commit to nursing school. Others stay in the role long-term because it fits their lifestyle, offers decent job security, and provides work that feels meaningful without the stress and responsibility level of licensed nursing. Not gonna lie, some facilities promote senior medication aides to supervisory or training roles, but advancement opportunities within the medication aide track are limited compared to nursing careers.
Why facilities mandate MACE certification
Legal liability drives facility requirements more than anything else, honestly. Medication errors can kill people. They can cause serious harm. They generate lawsuits, regulatory sanctions, and bad publicity. Requiring staff to pass a standardized competency exam provides some protection against claims of negligent hiring or inadequate training. It's not foolproof, but it demonstrates due diligence.
Regulatory compliance in many states now mandates certification. State surveyors check medication aide credentials during inspections. Facilities that employ uncertified staff for medication administration face citations, fines, and potential license restrictions. As more states move toward mandatory certification, facilities have no choice but to require it.
Quality of care improves when staff are properly trained and tested on medication administration. The medication aide competency exam ensures baseline knowledge about drug classifications, common side effects, proper techniques, and documentation standards. Does passing an exam guarantee someone will be a great medication aide? No. But it's better than having completely untrained people handling medications.
State variations and regulatory space
About 35 states currently require some form of medication aide certification, though they call it different things. Qualified Medication Administration Personnel (QMAP) in Colorado, Medication Technician in some states, Certified Medication Aide in others. The actual scope of practice, training requirements, and exam content vary significantly. Some states allow insulin administration after additional training, others don't. Some permit PRN medications, others restrict them to licensed nurses. The thing is, there's no real consistency.
Interstate reciprocity is inconsistent and frustrating. Moving from one state to another often means retraining and retesting, even if you've been a certified medication aide for years. A few states have reciprocity agreements, but most evaluate credentials on a case-by-case basis. This lack of standardization creates barriers for workers and complicates workforce mobility, similar to issues with CNA reciprocity but even messier because medication aide regulations are newer and less uniform.
Prerequisites before you can test
Minimum age requirements typically range from 18 to 21 depending on the state. Some states accept 18-year-olds, others require you to be older before you can be certified to administer medications. High school diploma or GED is standard in most states, though a few don't have formal education requirements.
Required training program hours vary from 40 to over 100 hours of combined classroom and clinical instruction. The pharmacology basics for medication aides portion covers drug classifications, routes of administration, measurement systems, and common medications in long-term care. Clinical hours give you hands-on practice under instructor supervision, usually in a nursing home or similar facility.
Background checks and employer sponsorship requirements exist in some states. You might need to be employed or have a job offer from a facility before you can take the exam. Criminal background checks screen for certain convictions that would disqualify you from working with vulnerable populations. The process can take weeks to months from start to finish, depending on how backed up your state is.
Testing format and what exam day looks like
The MACE exam questions typically number between 60 and 100, depending on which version your state uses. You'll see multiple-choice questions testing knowledge of medication administration procedures, dosage calculations, safety protocols, documentation requirements, and recognition of adverse effects. Some states include scenario-based questions where you have to apply knowledge to realistic situations.
Time limits usually range from 90 minutes to 2 hours. That's enough time if you've prepared properly, but not so much that you can sit there forever puzzling over questions you don't know. Testing centers enforce strict ID verification and security protocols. No phones, no notes, no talking. They're pretty serious about it.
Passing scores vary but typically fall in the 70 to 80 percent range. The MACE passing score might be a raw score (you need 56 out of 80 correct) or a scaled score (you need 75 on a scale that adjusts for question difficulty). Some states use criterion-referenced scoring where you must demonstrate competency in each content area, not just achieve an overall passing percentage.
Cost considerations and financial planning
The MACE exam cost typically ranges from 75 to 150 dollars for the exam itself, though this varies by state and testing provider. That's just the test fee. You'll also pay for the training program, which can run anywhere from 300 to over 1,000 dollars depending on whether you take it through a community college, private training company, or employer-sponsored program.
Background checks add another 30 to 50 bucks usually. If you need fingerprinting (some states require it), that's another 40 to 60 dollars. Study materials like textbooks, MACE study guide resources, MACE practice test subscriptions can add up to 50 to 100 dollars if you're buying everything new, though you can find free or cheap resources if you look around.
Retake fees apply if you don't pass on the first attempt. Most states charge the full exam fee again, though some offer a reduced retake rate. Multiple failures can get expensive quickly, which is why adequate preparation matters. Some employers reimburse exam and training costs, especially if they're sponsoring you or if you agree to work for them for a specified period after certification.
Study strategies and preparation timeline
How long to study depends on your background, honestly. If you're currently working as a CNA and have been around medication administration, you might need 2 to 4 weeks of focused study. If healthcare is brand new to you, plan on 6 to 8 weeks minimum to master the material. The pharmacology basics for medication aides section trips up a lot of people because you're learning drug names, classifications, and effects all at once.
Dosage calculations require math practice even if you're generally good at math. You'll need to convert between measurement systems (metric, household, apothecary), calculate doses based on weight or body surface area, and determine how many tablets or milliliters to give. Work through dozens of practice problems until the formulas become automatic. Like, muscle memory automatic.
Documentation and MAR practice should involve actually filling out sample medication administration records, not just reading about them. Many study guides include blank MAR forms you can practice with. Understanding charting conventions, how to document refused medications, and what constitutes complete documentation is key for both the exam and your actual job.
Finding quality study resources
The official candidate handbook from your state's testing authority or nursing board is your most important resource, hands down. It outlines exactly what's on the exam, what you're expected to know, and sometimes includes sample questions. Don't skip this document to jump straight into third-party study guides. That's a mistake I've seen people make.
Medication aide textbooks like "Medication Aide Certification Review" or similar titles provide thorough content review. Your training program probably used a textbook. Review it thoroughly. Focus on sections covering the five rights of medication administration, common medication classifications, proper techniques for different routes, and safety protocols.
Online practice tests help you identify weak areas and get comfortable with question formats. The MACE practice test you choose should include detailed rationales explaining why each answer is correct or incorrect. Random questions without explanations don't teach you much. Look for resources that let you create custom quizzes by topic so you can drill your weak areas.
Renewal requirements and maintaining certification
The MACE certification renewal cycle varies by state but typically runs 1 to 2 years. You'll need to submit renewal paperwork, pay a renewal fee (usually 25 to 75 dollars), and document that you've met continuing education requirements. Some states require 12 to 24 hours of CE annually, others require in-service training through your employer.
Employment verification might be required to show you're actively working in a medication aide capacity. If you let your certification lapse, reinstatement requirements can be stricter. You might need to retake the training program or exam depending on how long it's been expired. Don't let it lapse if you plan to keep working in the field, because getting it back is a hassle.
Staying current with scope of practice changes matters because regulations evolve. Your state might expand what medication aides can do, or restrict certain activities. Professional responsibility includes knowing your current legal scope, even if your employer asks you to do something outside it, which (the thing is) happens more than it should.
Similar standardized exams like the HESI-A2 or TEAS-Test serve as gateways to nursing programs if you eventually decide to pursue LPN or RN licensure. The PTCE pharmacy technician exam represents an alternative healthcare certification path if medication interests you but direct patient care doesn't.
MACE Exam Prerequisites and Eligibility Requirements
MACE? It's the Medication Aide Certification Examination. Basically the test that usually sits at the end of a state-approved medication aide course and proves you're capable of passing meds safely under whatever rules your state's got going on.
The thing is, the name "MACE" gets tossed around pretty loosely. Some states call it a medication aide competency exam, some contract with totally different testing vendors, and honestly some don't use the MACE label at all even though the job role's basically identical. Confusing much?
Who the MACE is for (Medication Aides/Medication Technicians)
This one's for people working as Medication Aides or Medication Technicians in long-term care, assisted living medication aide certification settings, group homes, and similar facilities where medication distribution happens daily but doesn't require full nursing licensure. Often you're already a CNA first. Sometimes you're a resident assistant getting cross-trained. Depends on the state.
What certification allows you to do (scope varies by state)
Your certification lets you administer certain medications to stable patients under supervision, and document it correctly. That scope varies a lot though. Some states allow oral, topical, eye/ear drops, inhalers. Others restrict PRNs, controlled substances, insulin, or anything that looks remotely like "assessment." You've gotta know your state's limits, because your training and your exam eligibility are tied directly to those limits.
Test Prep MACE (Medication Aide Certification Examination) questions come up constantly, but honestly? The hardest part for many candidates isn't the studying. It's getting eligible. Paperwork. Timelines that drag. Background checks that take forever. Random state rules that your coworker swears "don't matter" until they absolutely do and you're stuck reapplying.
Some requirements are basically universal across the board, showing up in nearly every state's eligibility checklist. Others? Wildly state-specific. You can lose months if you start the wrong program or assume reciprocity will transfer cleanly.
Minimum age, education, and ID requirements (state-specific)
Minimum age is typically 18.
Some states allow 16 to 17, but with restrictions like needing to be enrolled in a health pathway program, needing parental consent, or being limited to certain facilities or medication routes that don't involve controlled substances. Verify the exact age rule before you pay a tuition deposit. Refunds? Yeah, good luck with that.
Education requirement's often a high school diploma or GED. The verification process can be as simple as uploading a copy, or it can be "official transcript only" with the school seal. Annoying if you graduated years ago or changed your name since then. Alternative education documentation gets accepted sometimes, like foreign secondary education evaluation, adult education completion certificates, or proof of current enrollment, but only in certain jurisdictions.
You'll also need valid government-issued photo identification for exam registration and test day. That means a driver's license, state ID, passport, or other state-approved ID. Not a work badge. Not a screenshot. And yes, mismatched names are a real issue, so if your training certificate says "Katie" and your ID says "Katherine," fix it early.
Many boards require a Social Security number or taxpayer identification number for certification tracking, registry purposes, and background check matching systems. Sometimes it's for the state registry. Sometimes it's for background check matching. Either way, if you don't have it, you need to ask the state what the alternate path is. Some places simply won't issue certification without an SSN.
English language proficiency can be explicit or implicit depending on state policy. Some states require proof. Others don't, but the exam's in English and so are medication labels, MAR documentation and medication errors reporting forms, and facility policies. If you need accommodations, ask early. Testing vendors can allow approved accommodations, but you'll need paperwork and lead time.
Reading comprehension matters more than people think, honestly. Med labels are dense. "Hold for SBP < 100" is short, but if you don't know what it means you're sunk. Some training programs include a reading assessment, and some include a basic math skills assessment too. Dosage calculations and measurement basics are where many candidates struggle hard.
Physical ability also shows up as a prerequisite. Not "bench press 200 pounds," but being able to perform medication administration tasks safely, like standing, walking med carts, opening packaging, crushing meds properly, and using PPE correctly.
Residency rules vary wildly. Some states require you to be a resident. Others allow out-of-state candidates but require training within the state, or they require extra verification steps that add weeks to your timeline. Legal work authorization and citizenship documentation can be required by employers even if the state testing authority doesn't ask for it. Different gatekeepers, same outcome.
Required training program hours and clinical skills verification
State-mandated training hours typically land somewhere around 40 to 140 hours depending on jurisdiction. The breakdown matters.
Classroom instruction hours cover the core curriculum topics that show up everywhere: the rights of medication administration, infection control, storage and disposal, and legal/ethical guidelines and scope of practice. Clinical practicum hours are where you prove you can do the work without freezing up or making dangerous mistakes.
Pharmacology basics for medication aides is always in there. You won't become a pharmacist, obviously, but you need the basics of drug classifications and actions, common side effects, interactions, and what to report immediately. You'll also cover documentation and reporting, including MAR entries, late entries, refusals, and incident reporting.
Hands-on clinical experience requirements can include supervised medication passes under licensed nurse observation. Some programs require a minimum number of successful medication administrations documented during training, and that documentation has to match the state skills checklist exactly. Skills checklist verification and instructor sign-off requirements? Not "optional." If your instructor forgets to sign one box, your exam application can get rejected.
Training providers vary. Community colleges are common. Vocational schools too. Employer-based programs are huge in long-term care, especially when facilities are short-staffed and want to grow their own med aides instead of competing for certified candidates. Online vs. in-person options exist in some states, often as hybrid formats, but clinical skills still have to be verified in person.
You also need a training program completion certificate as a prerequisite for exam eligibility. There's usually a timeframe within which the exam must be taken after training completion, like 6 months or 12 months. Miss it, and you might need refresher training requirements or even to repeat the course. Not gonna lie, this is where people get burned because they finish training, get busy at work, and then realize their eligibility window expired.
Reciprocity? Total mess.
Reciprocity and transfer of training credits between states is messy at best. Some states accept prior training but require a state-specific bridge course. Others require you to challenge the exam only if you meet experience hours. Some just say no. If you're relocating, verify before you move, not after.
I was talking to someone last week who'd been a med aide in Ohio for three years, moved to Florida thinking it'd transfer automatically, and ended up having to take a 60-hour bridge course and pay for the whole thing herself because her facility wouldn't cover it. Three years of clean MAR sheets, zero errors, didn't matter. State wanted their hours documented their way.
Costs are part of prerequisites too. Tuition, books, uniforms, drug screen, immunization records, TB testing documentation, fingerprinting. People forget to budget for the extras, then delay the exam while they scrape together fees.
Background check and employer sponsorship (when applicable)
Clean criminal background is a common eligibility requirement. "Clean" doesn't always mean "no record," it means no disqualifying offenses under healthcare employment eligibility rules. Many states require fingerprinting procedures and run FBI vs. state-level background checks, plus healthcare-specific background screening like abuse registry checks. That registry check can be a dealbreaker even when a criminal case was minor or dismissed.
Timeframe for background check validity matters. Some states accept a check completed within the last 90 days. Others want it tied to a specific application. If your background check expires mid-process, you pay again. Fun.
There's often a process for appealing or explaining past criminal history. It can include court documents, letters of recommendation, proof of rehabilitation, and a waiting period after sentence completion. If this might apply to you, talk to the state authority early. Don't rely on a coworker's story from 2014.
Drug screening requirements show up a lot, usually on the employer side, but sometimes they're baked into training placement rules for clinical sites that won't accept students without negative screens. Health screening and immunizations can also be required by the clinical facility even if the state doesn't mandate them.
Who pays? Depends entirely. Some employers cover background checks and fingerprinting. Some make the candidate pay upfront then reimburse later. Some pay nothing. Employer vs. individual responsibility is a big deal here. You should ask in writing because people "promise" reimbursement all the time and then budgets change.
Employer sponsorship requirements exist in states where individual certification isn't fully portable between facilities. In a facility-based certification model, your authorization to pass meds is tied to that employer, that facility type, sometimes even that specific building. In a portable individual certification model, you're on a state registry and can take it with you. Big difference.
Employment verification and current job requirements can be part of exam eligibility depending on your state's model. Some states require you to be employed in a licensed facility. Some require supervisor or nurse attestation of competency and character references. Conditional eligibility and provisional certification options exist in a few places, like provisional employment during background check processing, but the rules are strict and the timelines are short.
State nurse aide registry status and good standing comes up constantly. If your CNA is expired, or you have a finding on the registry, that can block medication aide eligibility even if you completed training perfectly.
MACE exam objectives and content outline
Medication administration fundamentals is the "rights" stuff and the workflow that prevents errors from happening in the first place. Dosage calculations and measurement basics is where people miss points fast. Infection control and safety includes PPE, storage, disposal, and what to do with contaminated supplies.
Documentation and reporting covers MAR, refusals, omissions, and incident reporting. Know this cold. Recognizing side effects, adverse reactions, and emergencies shows up in scenario questions. Legal/ethical guidelines and scope of practice is basically "know what you can't do," because the exam loves that.
MACE exam cost and fees
People ask constantly, "How much does the MACE exam cost?" Typical exam fee ranges vary by state and vendor, often roughly $75 to $200, but that's not the full price of becoming eligible by any stretch. Additional costs include training program tuition, retakes, fingerprinting/background checks, and sometimes registry fees. Fee waivers are uncommon, but employer reimbursement is common enough that it's worth asking HR before you pay.
MACE passing score and scoring details
"What is a passing score on the MACE exam?" It's set by the state or testing authority. Some use scaled scoring which can be confusing when you're trying to figure out how many questions you can afford to miss. Retake rules and waiting periods are also state-specific. They can include limits like three attempts per year or mandatory remediation after a fail.
How difficult is the MACE exam?
"How hard is the MACE exam to pass?" If you can read carefully, do basic math, and you take MAR practice seriously, it's doable. Most failures come from math anxiety, rushing through scenario questions, and not understanding documentation rules in the state test plan.
Study time depends on experience. CNAs who have watched med passes usually need less time than someone brand new to healthcare. Everyone should practice calculations and label reading until it feels boring.
Best MACE study materials (Free + Paid)
The official candidate handbook and test plan? Best resource. Period. Pair it with a solid Medication Aide Certification Exam prep book that matches your state curriculum, plus pharmacology basics for medication aides chapters and a stack of dosage worksheets.
Flashcards help. A MACE study guide can help. Instructor-led reviews can help if you need structure, but self-study works fine if you're consistent.
MACE practice tests and sample questions
A good MACE practice test should match your state objectives and include rationales that explain why wrong answers are wrong, not just why right answers are right. Use timed sets, keep an error log, and drill weak areas. MACE exam questions that don't explain why an answer is right are basically entertainment, not prep.
MACE exam day tips (What to Expect)
Bring the exact ID required. Show up early, follow test center policies like no hats, no phones, no "just checking the time." Pacing matters, so don't camp out on one calculation question while the clock bleeds out.
Do a last-minute check of conversions, common abbreviations, and documentation rules. Then stop studying. Sleep.
MACE certification renewal requirements
"How do I renew my MACE certification and how often?" That's state-specific, naturally. Many require periodic renewal with a fee, continuing education or in-service hours, and employment verification. If you lapse, reinstatement might require a refresher course or re-testing.
Frequently asked questions about MACE test prep
"What should I study for the Medication Aide Certification Examination?" Focus on the state test plan, rights of administration, calculations, safety, and MAR documentation and medication errors prevention. Those areas consistently make up the bulk of exam content.
If you want one practical takeaway, it's this: verify your MACE exam prerequisites with your state authority before you start training. Prerequisites exist to make sure you're ready for safe medication administration training. The state will not bend the rules just because you already paid for the class.
Understanding what the MACE actually tests
The MACE study guide is basically your blueprint for passing this certification exam, and honestly it's not something you want to ignore. Look, I've seen people walk into this test thinking they can wing it because they've been passing meds in their training facility for months. That's a recipe for having to pay that exam fee all over again. The content outline breaks down into specific domains, each weighted differently. Understanding those percentages tells you where to focus your limited study time.
Most MACE exams divide content into six or seven major domains. Administration procedures usually take up about 35-40% of the questions. That's the biggest chunk by far. Documentation and reporting might be 15-20%. Dosage calculations typically run 10-15%, which sounds small but those math questions can absolutely tank your score if you're not prepared. Then you've got infection control and safety procedures at another 10-15%. Legal and ethical responsibilities usually account for 10-12% of exam content. Recognizing adverse reactions and side effects takes maybe 8-10%. Some test versions include a separate domain for communication, others fold it into the other sections.
The test blueprint exists for a reason. It's telling you exactly what percentage of questions comes from each area. If medication administration procedures is 40% of your exam and you only spend 10% of your study time on it because you think you already know it, you're setting yourself up for failure. I mean, it sounds obvious when I say it like that, but people do this constantly.
Why you can't skip the "easy" sections
Here's where candidates mess up.
They see a domain like "legal and ethical guidelines" and think oh I'll just use common sense on those questions. Wrong. The MACE doesn't test common sense. It tests whether you know specific regulations, state nurse practice acts, and the precise scope of practice for medication aides in your jurisdiction. You might feel super confident about medication administration because you've done it a hundred times during clinical training. But the exam asks about edge cases, contraindications, and situations you maybe haven't encountered yet.
Every domain connects to real-world medication aide responsibilities, but the exam focuses on critical decision points and safety protocols. When should you hold a medication and notify the nurse? What's the proper procedure when a resident refuses their medication? How do you document a PRN medication correctly? These aren't just theoretical questions. They reflect situations where medication aides commonly make errors that compromise patient safety.
The official test plan should be your primary study roadmap. Not some random YouTube video, not your friend's notes from last year. The official content outline published by your testing authority shows you exactly what's included and excluded from each domain. Some states use the D&S Diversified Technologies MACE, others use different testing vendors. The structure varies slightly, but the principle remains the same: study what they tell you they're going to test.
Cognitive complexity and question formats
The MACE tests multiple cognitive levels.
Recall questions are the easiest. They're asking you to remember a fact or definition. What are the six rights of medication administration? That's straight recall. Application questions give you a scenario and ask you to apply your knowledge. A resident has difficulty swallowing pills, what should you do? That requires you to apply proper techniques, not just recite them. Analysis questions are trickier. They might give you multiple pieces of information and ask you to determine what's most important or what action to take first.
Critical thinking questions often involve prioritization or recognizing complications, like when you're administering medications to four residents. One's complaining of chest pain, one refuses their medication, one needs a PRN pain medication, and one's ready for scheduled medications. What do you do first? These scenario-based questions trip people up because there's often more than one technically correct answer, but only one best answer according to safe medication administration training protocols.
Not all questions are scenario-based though. Plenty of straightforward knowledge questions exist too. What does PRN mean? List the rights of medication administration. What temperature range should refrigerated medications be stored at? You need both types of knowledge: the memorized facts and the ability to apply them in realistic situations.
How exam content reflects current practice standards
The MACE exam objectives align with current best practices in medication administration, not outdated protocols from twenty years ago. For 2026, some testing authorities have updated their exam content to reflect expanded scope of practice in certain states, increased emphasis on electronic MAR systems, and stronger focus on medication safety with high-risk populations. If you're studying from a textbook published in 2018, you might be missing important updates to infection control procedures, changes in controlled substance documentation requirements, or new standards for medication disposal.
Recent changes vary wildly by state.
Some states now allow medication aides to administer certain medications via additional routes they couldn't before. Others have added requirements for specific competencies like blood glucose monitoring or inhaler administration. Your exam content reflects what's legally permitted and currently practiced in your state, so a study guide from another state might not fully prepare you.
The relationship between training curriculum and exam content should be tight, but gaps exist. Your training program covers what the state requires for certification, and the exam tests that content. However, training programs sometimes emphasize certain topics more than others based on instructor preference or facility needs. The exam doesn't care what your instructor spent three weeks on. It tests according to the published content outline percentages.
The rights of medication administration in detail
The six rights of medication administration form the foundation of safe practice: right patient, right medication, right dose, right route, right time, and right documentation. Modern practice recognizes additional rights though. Right to refuse means residents can decline medications and you must respect that autonomy while documenting properly and notifying appropriate personnel. Right reason means understanding why the medication's prescribed. You should know whether this is for blood pressure, pain, infection, or something else. Right response involves monitoring for therapeutic effects and adverse reactions after administration.
Verification procedures aren't optional.
You check the MAR against the medication label three times minimum: when you take it from storage, when you prepare it, and before you administer it. You verify patient identity using two identifiers, never just the room number. You confirm the dose matches what's ordered, the route's appropriate, and the timing falls within acceptable administration windows.
Reading and interpreting physician orders accurately is critical, like when an order might say "Metoprolol 25mg PO BID" and you need to understand that's 25 milligrams by mouth twice daily. Medication labels contain multiple pieces of information: generic name, brand name, strength, total quantity, expiration date, special storage instructions, and warnings. MACE exam questions frequently test whether you can extract the correct information from a label and match it to an order.
I had a coworker once who got written up because she kept confusing BID with TID. Gave medications three times a day instead of two for an entire week before someone caught it. The resident was fine, but it could have been serious depending on the medication. That's the kind of basic knowledge that feels too simple to study, but it matters.
Routes of administration and proper technique
Understanding medication routes goes way beyond knowing oral means by mouth. Oral medications include tablets, capsules, and liquids. Topical means applied to skin. Transdermal patches deliver medication through skin over time. Ophthalmic goes in the eyes, otic in the ears. Nasal medications go in the nose, rectal suppositories in the rectum, vaginal suppositories or creams in the vagina. Each route requires specific technique to ensure safety and efficacy.
Proper techniques matter enormously. For oral medications, you position the patient upright or at least at a 45-degree angle to prevent aspiration. You stay with them until they swallow the medication. Never leave pills at the bedside. For eye drops, you pull down the lower lid and drop into the conjunctival sac, never directly onto the eyeball. For ear drops, you pull the ear up and back for adults, down and back for children. These specifics show up on the exam.
Positioning patients appropriately prevents complications.
A resident who can't sit up for oral medications is at aspiration risk. Someone receiving rectal medications needs to be positioned on their left side for proper insertion and retention. Transdermal patches go on clean, dry, hairless skin in rotating sites to prevent irritation.
Assisting patients who have difficulty swallowing requires specific strategies. You might thicken liquids to an appropriate consistency, offer small sips of water between bites, or use specialized cups with cutouts for the nose. Crushing medications is sometimes necessary but has strict rules. Extended-release, enteric-coated, and sublingual medications should never be crushed. Capsules generally shouldn't be opened unless specifically designed for that. When crushing's appropriate, use a proper pill crusher, mix with a small amount of soft food immediately before administration, and ensure the entire dose is consumed.
Mixing medications with food or beverages requires knowledge of compatibility. Some medications must be taken on an empty stomach, others with food. Certain drugs interact with dairy products, grapefruit juice, or high-fiber foods. You need to know resident preferences too. Nobody wants their pills mixed in their favorite pudding if it ruins the taste.
Time-sensitive medications and PRN protocols
Time-sensitive medications have specific administration windows. Scheduled medications are typically given within 30 minutes before or after the ordered time, though this varies by facility policy and medication type. Critical medications like insulin or antibiotics might have tighter windows. You document the actual administration time, not the scheduled time.
PRN medications require assessment before administration. A resident requests pain medication, so you assess their pain level, check when the last dose was given, verify you're within the allowable frequency, and evaluate whether the medication's appropriate for the situation. After administration, you document why it was given, the time, and you follow up to assess effectiveness. Did their pain decrease? By how much? This information guides future care decisions.
Special populations and communication strategies
Medication administration in special populations demands adapted approaches. Elderly residents often take multiple medications, have slower metabolism, and are more sensitive to side effects. Cognitively impaired residents might not understand why they're taking medications or might forget they already took them. Developmentally disabled individuals might have sensory sensitivities or communication barriers that affect medication administration.
Cultural considerations matter.
Some cultures have beliefs about certain medications or administration routes. Religious practices might affect timing or type of medications acceptable. Respecting these preferences while ensuring necessary medications are given requires communication and sometimes creative problem-solving with the healthcare team.
Communication techniques for resistant or confused residents include offering choices when possible, explaining in simple terms what the medication does, using distraction or redirection, and never forcing medications. If a resident consistently refuses, you document and notify the nurse. There might be underlying reasons like difficulty swallowing, nausea, or side effects they're experiencing but can't articulate.
Math skills and dosage calculations
MACE exam questions frequently test basic dosage calculation skills, and this is where people either sail through or completely bomb. Converting between measurement systems means knowing that 1 teaspoon equals 5 milliliters, 1 tablespoon equals 15 milliliters, and 1 ounce equals 30 milliliters. The metric system uses grams, milligrams, and micrograms with consistent conversion factors. The apothecary system (grains, drams) is mostly obsolete but occasionally appears on older exam versions.
Calculating tablet dosages when splitting or combining tablets requires careful math. If the order's for 7.5mg and you've got 5mg tablets, you need 1.5 tablets. If you've got 15mg tablets, you'd need half a tablet. But wait, can that tablet be split? If it's not scored, you can't split it accurately. This kind of critical thinking accompanies the calculation.
Liquid medication measurement using medication cups requires reading calibration marks at eye level at the bottom of the meniscus. Oral syringes provide more accurate measurement for small volumes. Droppers vary by design, so you need to use the dropper that comes with the specific medication.
Reading calibration marks accurately sounds simple but errors happen constantly. Is that line 7.5mL or 8mL? Double-check. Calculating dosages based on weight rarely comes up for medication aides since those calculations are typically done by pharmacists or nurses, but understanding the concept helps you recognize when a dose seems wrong.
Understanding medication concentrations means knowing that 250mg/5mL is different from 125mg/5mL. The first is more concentrated. If you're measuring a 250mg dose, you'd need 5mL of the first solution but 10mL of the second. Proportion and ratio methods work well for these calculations. Set up the known concentration as a ratio, then solve for the unknown volume.
Decimal and fraction math skills are essential.
You need to multiply, divide, add, and subtract decimals accurately. Rounding rules matter. Generally round to the nearest tenth for liquid medications, but some facilities have specific policies. When in doubt about a calculated dose, ask. An unreasonable dose like 47 tablets or 0.02 tablets signals a calculation error. Go back and check your work.
Common calculation errors include misplacing decimal points, confusing milligrams with micrograms, using the wrong concentration, or setting up proportions incorrectly. When to ask the nurse for assistance? Anytime you're unsure, anytime the calculation seems off, or anytime you're dealing with a high-alert medication. Better to ask than to make a potentially fatal error.
If you're looking for structured preparation similar to other standardized tests like the TEAS-Test or HESI-A2, consider using dedicated practice materials. Our MACE Practice Exam Questions Pack offers realistic questions covering all these calculation scenarios.
Infection control and medication safety
Standard precautions and hand hygiene before and after medication administration are non-negotiable. Wash hands or use alcohol-based hand sanitizer before preparing medications, between residents, and after completing your medication pass. This prevents cross-contamination and protects vulnerable populations.
Personal protective equipment use when handling medications depends on the situation. Gloves are required for topical, rectal, or vaginal administration. If there's risk of splash or spray, eye protection might be necessary. When handling medications for residents with certain infections, additional PPE might be needed according to transmission-based precautions.
Proper storage of medications includes maintaining temperature requirements. Most medications are stored at room temperature (68-77°F), but some require refrigeration (36-46°F). Light-sensitive medications need dark storage. Humidity-sensitive medications shouldn't be stored in bathrooms. Following manufacturer guidelines prevents medication degradation and maintains efficacy.
Securing medications prevents unauthorized access or diversion.
Medication carts must be locked when unattended, even for a moment. Controlled substances require double-lock systems, locked within a locked cart or cabinet. Medication rooms should be locked when not in use. These security measures protect residents from accidental ingestion and prevent theft or misuse.
Controlled substance storage and handling has strict regulations. You must count controlled substances at shift change, document each dose administered, and report discrepancies immediately. Some states require two staff members to witness controlled substance administration or disposal.
Expiration date monitoring and removing outdated medications is an ongoing responsibility. Check dates regularly, usually monthly, and remove expired medications from active storage immediately. Follow facility policy for returning them to pharmacy or disposing properly. Never administer expired medications because potency and safety can't be guaranteed.
Proper disposal of unused, expired, or discontinued medications follows EPA and DEA guidelines. Most facilities use pharmaceutical waste containers or medication take-back programs. Never flush medications down the toilet (except specific drugs on the FDA flush list) or throw them in regular trash. Sharps disposal containers are required for lancets used in blood glucose monitoring, even though medication aides don't typically handle needles for injections.
Documentation standards and error prevention
MAR documentation can't be overstated.
Incomplete or inaccurate documentation is a leading cause of medication errors. Completing medication administration records immediately after giving medications prevents omissions and duplications. If you document before administering and then the resident refuses or an emergency occurs, your record's false.
Required elements of MAR documentation include date, time (actual time of administration, not scheduled time), your initials, and a signature key linking your initials to your full name and title. Some MARs require additional information like blood pressure or blood glucose readings for certain medications.
Documenting refused medications and reasons for refusal protects everyone. Note that the resident refused, document the stated reason if they provide one ("said it makes her dizzy"), and notify the nurse according to facility policy. Never chart a medication as given if it wasn't.
Recording PRN medications requires more detail than scheduled medications. Document the reason given ("resident complained of headache, rated 7/10"), time administered, and effectiveness evaluation ("reassessed 30 minutes later, pain now 3/10"). This creates a record of appropriate PRN use and helps identify patterns.
Correcting documentation errors properly means drawing a single line through the error, writing "error" and your initials, then recording the correct information. Never use correction fluid, never scribble out entries, and never backdate documentation. In electronic systems, corrections create an audit trail showing what was changed and when.
Electronic MAR systems and barcode medication administration are becoming standard. You scan the medication barcode and the resident's wristband barcode, and the system verifies it's the right medication for the right person. This technology reduces errors but doesn't eliminate the need for your critical thinking. If the system alerts you to a problem, investigate. Don't override warnings without understanding why they occurred.
Recognizing and responding to medication effects
Common side effects of frequently administered medication classes should be familiar. Antihypertensives can cause dizziness and falls. Diuretics increase urination and can cause dehydration. Pain medications can cause constipation and drowsiness. Antibiotics might cause diarrhea or allergic reactions. Knowing expected side effects helps you distinguish them from serious adverse reactions.
The difference between expected side
What the MACE (Medication Aide Certification Examination) is
Test Prep MACE (Medication Aide Certification Examination) is the test a lot of states use to verify you can safely pass meds in places like assisted living and long term care, without pretending you're a nurse. Big deal. Real responsibility.
Medication aides and medication technicians take it when their state allows a non-nurse role to administer certain medications under a nurse's delegation or facility policy. Scope varies hard by state. One state might allow more routine oral meds, another might limit you to very specific tasks and require a tighter supervision setup for assisted living medication aide certification, which makes the whole thing confusing when you're trying to figure out what you can actually do after you pass.
This is for people already in care roles. CNAs. Med techs. Sometimes caregivers moving up.
If your state calls it a medication aide competency exam and not "MACE," the exam content's still usually the same vibe: safe medication administration training, basic pharmacology, and a lot of "what would you do next" scenarios. You know the type.
You'll typically be allowed to administer certain meds and document them. That includes MAR documentation and medication errors reporting, which is where people get sloppy when they're nervous.
Extra rules exist. Extra forms. Extra fees in some states. Keep reading.
Requirements change by state and testing provider, so don't assume your coworker's checklist is your checklist.
Age minimum's usually 18. Education's often a GED or high school diploma. IDs must match your registration name exactly, and yes, a missing middle initial can turn into a stupid administrative correction fee. Annoying little fragments everywhere.
Training hours vary, but most states expect a state-approved medication aide course plus clinical skills verification, and sometimes employer sponsorship. Background checks are common. Fingerprinting's where the "surprise $60" shows up for a lot of people.
Bring the right ID. Two forms sometimes. Read the candidate bulletin.
Name match matters. If you recently got married or changed your name, budget for name change processing, because some boards charge for it and some testing vendors do too. My cousin dealt with this last year after her wedding and ended up paying twice what she expected just to get her paperwork aligned.
Training can be quick or a grind depending on your state. A program might be 24 to 60+ hours with skills sign-offs, plus practice on MARs, crushing rules, storage, and documentation.
Background check and fingerprinting fees usually run $30 to $100. Drug screening might be required by the training program or your employer, and that's another $25 to $60-ish depending on where you live.
The test content usually hits safe administration, the "rights," basic calculations, infection control, documentation, adverse reactions, and legal scope. It's not trying to trick you, but it does punish guessing when you don't know the workflow.
Medication administration fundamentals (rights of medication administration)
Expect the rights, timing windows, and what to do when something doesn't match the order. Also, common med forms. Tablets. Liquids. Topical. PRN rules.
Dosage calculations and measurement basics
This is where people freeze. Conversions. mL to teaspoons. Counting tabs. Not complex algebra, but you've gotta be consistent.
Infection control and safety (PPE, storage, disposal)
Storage temps, controlled substances handling at a policy level, proper disposal, gloves, and what to do after exposure. Basic stuff, but tested.
Documentation and reporting (MAR, incident reporting)
MAR documentation and medication errors questions show up a lot, because facilities get cited for this stuff. You'll see scenarios like "resident refused" or "held for vitals" and what you document and who you notify.
Recognizing side effects, adverse reactions, and emergencies
This is your "call the nurse now" section. Allergic reaction signs, hypoglycemia symptoms, over-sedation. Stuff you can't miss.
Legal/ethical guidelines and scope of practice
Delegation rules. What you can't do. When you must escalate. State law drives this.
What you'll pay and why it varies
The standard MACE exam cost's typically $75 to $150, depending on the state and testing provider. That base exam fee usually covers test administration, scoring, and your initial score report, which is often electronic now.
Regional variation's real. Some states bake state registry processing into the exam fee, others split it into separate charges, so the sticker price looks lower until you hit checkout and see admin fees, registration processing fees, and sometimes a testing center surcharge for computer-based testing that nobody warned you about.
Typical exam fee range and what it includes
Base fee: $75 to $150. Most candidates land around the middle.
What it usually includes:
- sitting for the exam at an approved site
- scoring and pass/fail decision
- initial score report, often online
What it may not include is the stuff that makes you mutter at your screen. Printed score report options can cost extra, and duplicate score reports or certification verification fees can show up later when an employer asks for proof yesterday. Expedited results delivery sometimes exists, and it costs more, and it's only worth it if a job offer's waiting on your result.
Extra fees candidates forget to budget for
Hidden costs are where budgets fall apart. The exam fee's the easy part to Google. The rest? Death by small charges.
Here's the stuff I see people overlook, with two worth explaining and the rest you should at least pencil in:
- Registration processing fees and administrative charges: some vendors add $5 to $25 at checkout, and it feels petty, but it's common and it changes your real MACE exam cost.
- Scheduling fees and rescheduling penalties: if you miss the deadline or reschedule late, you might pay $10 to $50, and if you no-show you may lose the entire exam fee, which is brutal when you're living paycheck to paycheck.
- Late registration fees
- Testing center fees or computer-based testing surcharges
- State registry listing fees and initial certification processing
- Official certification card or certificate issuance fees
- Accommodation request processing for candidates with disabilities, not always a fee, but extra paperwork and sometimes extra documentation costs
- Address updates, admin corrections, name changes
- Retake fees, usually same as initial fee, sometimes slightly reduced
Total investment from training through certification
Medication aide training program tuition's usually $300 to $1,500 depending on provider and state. Training materials like textbooks, workbooks, and supplies run $50 to $200. Uniform requirements and clinical supplies can add another $30 to $150, depending on what they make you buy and whether you already own scrubs and shoes.
Then add background check and fingerprinting at $30 to $100, possible physical exam and immunizations if the program requires it, and drug screening if required. Study materials matter too. A decent MACE study guide plus a MACE practice test resource often runs $20 to $100, and yes you can pass without paying for extras, but you need enough MACE exam questions to stop making the same mistakes.
Thing is, if you want a paid set that's focused and not full of fluff, the MACE Practice Exam Questions Pack is $36.99, and it's the kind of thing you run timed when you're trying to lock down your weak areas.
Travel's another sneaky one. If the nearest testing center's far, budget gas, parking, maybe a hotel. And time off work's a cost even if it's not a line item, because training hours plus test day can mean lost shifts.
Total estimated cost for initial certification usually lands around $500 to $2,000 depending on your state, your training tuition, and whether you need extra medical clearances.
Payment methods, refunds, and cancellation rules
Most testing authorities take online card payments. Credit and debit. Some also accept checks or money orders for paper applications, and a few allow employer payment arrangements for group testing discounts.
Refunds. Not gonna lie, refunds are where people get mad. Many testing vendors treat exam fees as nonrefundable once you schedule, and cancellations might only get you a partial refund if you cancel early enough. Miss your appointment and you often forfeit the fee. Read the policy before you click submit, because "I didn't know" doesn't get your money back.
Some training providers offer payment plans for tuition, and occasionally installment payment plans for exam fees exist, but it's not universal.
How MACE fees compare to other healthcare cert costs
Compared to CNA state exams, MACE's often in the same general range for the exam itself, but the total spend can be higher once you count training tuition and registry processing. Compared to phlebotomy or EMT? MACE is usually cheaper overall, mostly because the training's shorter and you're not buying as much equipment, but it can still sting if you're paying everything out of pocket.
ROI: salary increase after certification
The return on investment's usually decent if your facility pays medication aides more than CNAs or caregivers. Some places bump hourly pay by $1 to $3, sometimes more, and you may get more consistent hours because meds have to be passed every day. The real ROI depends on whether your employer actually uses you in the med aide role after you certify, which is why I always tell people to ask that up front. During hiring or during the "will you sponsor me" conversation.
If you're negotiating an offer, ask for reimbursement after you pass, or up-front coverage with an employment commitment requirement. Workforce development grants, state-funded training programs, and even fee waivers for low-income candidates exist in some areas, plus veterans benefits and military tuition assistance if you qualify. Also, job-related education expenses can sometimes be tax deductible, so keep receipts and ask a tax pro.
Practical budgeting tips that actually help
Start with the known numbers. Training tuition. Background check. Exam fee.
Then add a buffer, because rescheduling happens, and retakes happen, and printed paperwork requests happen when HR's being HR. If you want a targeted practice option, slot in the MACE Practice Exam Questions Pack at $36.99 and treat it like insurance against a retake fee, because one retest can cost more than your study materials.
Quick FAQs people ask anyway
How much does the MACE exam cost? Typically $75 to $150, plus admin and state processing fees depending on where you test.
What's a passing score on the MACE exam? Your state or testing authority sets the MACE passing score, so check the candidate handbook for the exact number and whether it's scaled.
How hard's the MACE exam to pass? Moderate, mostly because calculations, terminology, and scenario questions trip people up when they rush.
What should I study for the Medication Aide Certification Examination? Focus on the official test plan, med rights, dosage basics, infection control, MAR documentation and medication errors, and practice with realistic MACE exam questions. A solid MACE study guide plus a MACE practice test routine helps.
How do I renew my MACE certification and how often? MACE certification renewal's usually every 1 to 2 years, with renewal fees around $25 to $75 and continuing education costs often $50 to $200 annually, depending on your state and employer setup. Optional professional liability insurance runs about $50 to $150 a year if you want it.
If you're pricing this whole thing out, do it like a grownup spreadsheet. Training. Exam. Admin stuff. Renewal. And one line for "random nonsense." That last line gets used more than you'd think.
What determines if you pass or fail
No universal number here. Most states? They're setting the bar somewhere between 70-80% correct answers, but honestly it depends on your specific state regulatory board. This isn't like the SAT-Test where you get a standardized national score. Medication aide certification falls under state nursing boards or health departments, and they each get to decide what constitutes minimum competency for safe medication administration.
The testing authority uses what's called a criterion-referenced approach, which means you're measured against a fixed standard of knowledge rather than competing against other test-takers. You either know enough to safely give medications to residents or you don't. Some states might require 75% overall, but also mandate you hit certain minimums in each content domain. Like you can't bomb the dosage calculations section even if you ace everything else. Period.
How your performance actually gets evaluated
Here's where it gets technical. Most MACE exams use scaled scoring rather than just counting up your raw score, which is literally the number of questions you got right. But the scaled score? That's a conversion that accounts for slight differences in difficulty between different exam forms.
Why does this matter? Because not everyone gets the exact same test. I mean, the testing company creates multiple versions to prevent cheating and maintain security. Through statistical equating procedures, they make sure a 75 on one version is equivalent to a 75 on another version, even if one had slightly harder questions. Similar to how standardized tests like the GRE-Test handle multiple forms.
Computer-based MACE exams typically give you immediate pass/fail notification. You'll see that result on screen right after you finish, but that's preliminary. Your official score report takes anywhere from 1-5 business days to process depending on the testing vendor. The one that goes to your state registry. Paper-based exams? You're waiting weeks.
There's typically no penalty for guessing wrong, so unanswered questions count the same as incorrect ones. Always fill in something. I've seen people waste time agonizing over skipped questions when they could've just made an educated guess and moved on. My cousin actually left twelve questions blank on her first attempt because she wanted to "be honest" about what she knew. She failed by nine points.
Score reports and what they actually tell you
Honestly? When you get your official score report, it breaks down your performance by content area, showing percentage correct in sections like medication administration fundamentals, dosage calculations, infection control, documentation, and recognizing adverse reactions. This breakdown is the most valuable part if you don't pass the first time.
Let's say you scored 82% on medication rights and safety protocols but only 58% on dosage calculations. That tells you exactly where to focus your remediation. Some reports also show whether you performed below, at, or above the passing standard in each domain, even if they don't give you exact percentages.
The score report doesn't typically include percentile ranks. Why? Because remember, this is criterion-referenced testing. Whether 90% of people passed or 40% passed doesn't change what you need to know. You're not competing against other candidates. You're demonstrating competency against an established standard.
How passing standards get established and reviewed
State boards don't just pull passing scores out of thin air. They typically convene panels of subject matter experts like experienced medication aides, nursing supervisors, educators. These folks go through a standard-setting process where they review each question and determine what a minimally competent medication aide should know.
The process often involves something called the Angoff method or similar procedures where experts estimate the probability that a barely competent candidate would answer each question correctly, then those probabilities get aggregated to set the cut score. It sounds complicated but the goal is straightforward: ensure anyone who passes can safely administer medications without harming residents.
Passing standards get periodically reviewed, usually every 3-5 years or when there are significant changes to medication aide scope of practice or regulations. If your state updates its passing score, you'll get notified through official channels like the state board website and testing vendor announcements. But changes are rare and usually minor, like adjusting from 73% to 75%.
Comparing pass rates across different contexts
Pass rates vary wildly. Some states report 85-90% first-time pass rates, others hover around 65-70%. This doesn't necessarily mean some states have easier exams. It often reflects differences in training program quality, prerequisite requirements, and candidate preparation levels.
States with more rigorous training hour requirements like 100+ hours of instruction plus clinical practice tend to have higher pass rates. Makes sense, right? Better prepared candidates perform better. Testing periods also matter. Summer testing windows often see slightly lower pass rates because that's when a lot of new grads from training programs all test at once, including those who barely scraped through their coursework.
Geographic variation is real too. Urban testing centers sometimes show different patterns than rural ones, possibly reflecting differences in training program resources and candidate demographics. But honestly, these statistics don't mean much for your individual preparation. Focus on mastering the content, not on what percentage of people passed last quarter.
What happens when you don't make the cut
Failed by one or two questions? I feel you, but a close fail is still a fail. You'll need to retest, and most states mandate a waiting period between attempts. Typically 30 to 90 days depending on state regulations.
This waiting period isn't arbitrary punishment. It's meant to give you time for meaningful remediation rather than just immediately retaking the same exam hoping for better luck. Many states also require proof of additional training or remedial coursework if you fail multiple times. After your second or third failure, you might need to complete another training program or supervised clinical hours before testing again.
There's usually a maximum number of attempts allowed within a specific timeframe. Some states cap it at three attempts per year, others have different rules, so check your state board requirements because violating these policies can complicate your certification path. Similar to healthcare licensing exams like the NAPLEX, there are real consequences for not following retesting protocols.
Using scoring information to set realistic study goals
Once you understand the passing score and content domain breakdown, you can build a targeted study plan. If you need 75% overall and the exam has 100 questions, you can miss 25 and still pass. But don't aim for exactly 75%. Give yourself a buffer. Target 80-85% in your practice tests.
Pay attention to which domains carry more weight. If medication administration procedures account for 35% of the exam and dosage calculations are 20%, you know where to allocate study time. Use your practice test results the same way you'd use official score reports. Identify weak areas and drill them repeatedly.
The score validity period varies by state. Most require you to actually get employed as a medication aide and start working within 12-24 months of passing. Your passing score doesn't expire exactly, but your eligibility to be certified might if you don't complete all requirements within a certain window. Not like the MCAT-Test where scores are valid for years regardless of what you do with them.
Look, understanding MACE scoring isn't just about knowing the magic percentage you need. It's about recognizing that this exam measures whether you're safe to administer medications to vulnerable populations. The passing standard represents the minimum knowledge required for that responsibility. Approach your preparation with that mindset, and the score will take care of itself.
Conclusion
Getting your medication aide certification isn't optional if you want to work
You already know.
The MACE exam stands between you and actually working as a medication aide in most states, and honestly, the exam cost ranges from about $65 to $120 depending on where you test. That's not even the expensive part if we're being real here. It's the training hours and background checks that add up. But here's the thing. You can't skip this. No certification means no job in assisted living facilities, no administering medications, no career advancement beyond basic CNA work.
The MACE passing score varies by state but usually hovers around 75-80% of questions answered correctly, which sounds manageable until you're staring at dosage calculation questions under time pressure or trying to remember the difference between a side effect and an adverse reaction. Wait, or was it.. yeah, you see what I mean. The exam isn't impossibly hard, but it's not a joke either. Medication administration fundamentals, MAR documentation, infection control protocols, pharmacology basics for medication aides. You need all of it down cold.
Study time? Three to six weeks.
Most people study 3-6 weeks if they've already finished their training program. Less time if you're fresh out of class, more if you've been out of the healthcare field for a while or struggle with math. The key is practice questions. Not reading the same study guide five times. Not rewatching your instructor's videos. Actual MACE practice test questions that mimic what you'll see on exam day.
Safe medication administration training only sticks when you apply it repeatedly to scenario-based questions that test whether you really understand the "why" behind each medication error prevention step. Flashcards help with terminology. Dosage calculation worksheets build confidence with math. But practice exams show you where your knowledge gaps actually are, not where you think they are. Big difference there. I've seen people who swore they had infection control nailed completely bomb that section because they memorized procedures without understanding the reasoning.
When you're ready to test your readiness seriously, the MACE Practice Exam Questions Pack gives you the question volume and answer explanations you need to identify weak areas before they cost you on test day. Real exam-style questions, detailed breakdowns, the kind of prep that shows you what "recognizing adverse reactions" or "assisted living medication aide certification scope" actually means in a testing scenario.
Your MACE certification renewal comes every 1-2 years depending on your state, so this isn't a one-and-done thing. But passing the first time? That's what gets you working, earning, and building the experience you need for the long run. Study smart, practice hard, and don't walk into that test center guessing.
Show less info
Comments
Hot Exams
Related Exams
WorkKeys Assessment
Pharmacy College Admission Test
American College Testing: English, Math, Reading, Science, Writing
Pre-Professional Skills Test (PPST) - Writing Section
Advanced Cardiac Life Support
National Registry Emergency Medical Technician
Chartered Financial Analyst Level 1
CLEP Science and Mathematics: Biology, Calculus, Chemistry, College Algebra & Mathematics, Precalculus, Natural Sciences
Law School Admission Test: Logical Reasoning, Reading Comprehension, Analytical Reasoning
North American Pharmacist Licensure Examination
Georgia Assessments for the Certification of Educators
Emergency Medical Technician
Computer-adaptive Placement, Assessment, and Support System: English, Math, Writing
HESI Admission Assessment Exam (A2)
California Basic Educational Skills Test - Reading
Short Placement Tests Developed by ACT
How to Open Test Engine .dumpsarena Files
Use FREE DumpsArena Test Engine player to open .dumpsarena files

DumpsArena.co has a remarkable success record. We're confident of our products and provide a no hassle refund policy.

Your purchase with DumpsArena.co is safe and fast.
The DumpsArena.co website is protected by 256-bit SSL from Cloudflare, the leader in online security.